[{"id":"276","chapterid":"749","timeTo":"195.26 ","timeFrom":"0 ","number":"1","chaptername":"Introduction of session ","description":" "},{"id":"276","chapterid":"789","timeTo":"243.914 ","timeFrom":"195.261 ","number":"2","chaptername":"First live endoscopy: \"How I perform gastroscopy\" ","description":"Introduction of case "},{"id":"276","chapterid":"790","timeTo":"296.256 ","timeFrom":"243.915 ","number":"3","chaptername":"First inspection of oesophagus and GOJ ","description":" "},{"id":"276","chapterid":"791","timeTo":"344.267 ","timeFrom":"296.256999","number":"4","chaptername":"Inspection of stomach ","description":" "},{"id":"276","chapterid":"792","timeTo":"511.917 ","timeFrom":"344.268 ","number":"5","chaptername":"Inspection of bulb and duodenum ","description":" "},{"id":"276","chapterid":"793","timeTo":"725.314 ","timeFrom":"511.917999","number":"6","chaptername":"Retroflexion in stomach ","description":" "},{"id":"276","chapterid":"794","timeTo":"1022.501 ","timeFrom":"725.314999","number":"7","chaptername":"Second inspection of oesophagus ","description":" "},{"id":"276","chapterid":"795","timeTo":"1440.689 ","timeFrom":"1022.502 ","number":"8","chaptername":"Discussion with moderators ","description":" "},{"id":"276","chapterid":"796","timeTo":"1947.216 ","timeFrom":"1440.69 ","number":"9","chaptername":"Second live endoscopy: \"Lesion Characterisation at Upper GI\" ","description":" "},{"id":"276","chapterid":"797","timeTo":"2242.549 ","timeFrom":"1947.21699","number":"10","chaptername":"Surprising detection of neoplastic lesion ","description":" "},{"id":"276","chapterid":"798","timeTo":"2419.284 ","timeFrom":"2242.55 ","number":"11","chaptername":"Discussion with moderators ","description":" "}]
[{"id":"276","split":"1","chapterid":"749","timeFrom":"0 ","timeTo":"195.26 ","number":"1","chaptername":"Introduction of session ","description":" ","tagid":"569","tagName":"GIEQs Digital Edition I"},{"id":"276","split":"1","chapterid":"790","timeFrom":"243.915 ","timeTo":"296.256 ","number":"3","chaptername":"First inspection of oesophagus and GOJ ","description":" ","tagid":"369","tagName":"Assessment of the gastro-oesophageal junction"},{"id":"276","split":"1","chapterid":"790","timeFrom":"243.915 ","timeTo":"296.256 ","number":"3","chaptername":"First inspection of oesophagus and GOJ ","description":" ","tagid":"174","tagName":"Tip attachments"},{"id":"276","split":"1","chapterid":"790","timeFrom":"243.915 ","timeTo":"296.256 ","number":"3","chaptername":"First inspection of oesophagus and GOJ ","description":" ","tagid":"260","tagName":"Oesophagus"},{"id":"276","split":"1","chapterid":"791","timeFrom":"296.256999","timeTo":"344.267 ","number":"4","chaptername":"Inspection of stomach ","description":" ","tagid":"370","tagName":"Benefit of simethicone"},{"id":"276","split":"1","chapterid":"791","timeFrom":"296.256999","timeTo":"344.267 ","number":"4","chaptername":"Inspection of stomach ","description":" ","tagid":"261","tagName":"Stomach"},{"id":"276","split":"1","chapterid":"792","timeFrom":"344.268 ","timeTo":"511.917 ","number":"5","chaptername":"Inspection of bulb and duodenum ","description":" ","tagid":"368","tagName":"Visualisation of posterior wall of D2 and junction"},{"id":"276","split":"1","chapterid":"792","timeFrom":"344.268 ","timeTo":"511.917 ","number":"5","chaptername":"Inspection of bulb and duodenum ","description":" ","tagid":"366","tagName":"Gastroscope handling"},{"id":"276","split":"1","chapterid":"792","timeFrom":"344.268 ","timeTo":"511.917 ","number":"5","chaptername":"Inspection of bulb and duodenum ","description":" ","tagid":"262","tagName":"Duodenum"},{"id":"276","split":"1","chapterid":"792","timeFrom":"344.268 ","timeTo":"511.917 ","number":"5","chaptername":"Inspection of bulb and duodenum ","description":" ","tagid":"367","tagName":"Visualisation of the major papilla"},{"id":"276","split":"1","chapterid":"793","timeFrom":"511.917999","timeTo":"725.314 ","number":"6","chaptername":"Retroflexion in stomach ","description":" ","tagid":"500","tagName":"Retroflexion in the stomach (J manouevre)"},{"id":"276","split":"1","chapterid":"793","timeFrom":"511.917999","timeTo":"725.314 ","number":"6","chaptername":"Retroflexion in stomach ","description":" ","tagid":"499","tagName":"Hill Classification"},{"id":"276","split":"1","chapterid":"793","timeFrom":"511.917999","timeTo":"725.314 ","number":"6","chaptername":"Retroflexion in stomach ","description":" ","tagid":"497","tagName":"Describing position within the stomach"},{"id":"276","split":"1","chapterid":"793","timeFrom":"511.917999","timeTo":"725.314 ","number":"6","chaptername":"Retroflexion in stomach ","description":" ","tagid":"306","tagName":"Virtual chromoendoscopy"},{"id":"276","split":"1","chapterid":"793","timeFrom":"511.917999","timeTo":"725.314 ","number":"6","chaptername":"Retroflexion in stomach ","description":" ","tagid":"369","tagName":"Assessment of the gastro-oesophageal junction"},{"id":"276","split":"1","chapterid":"793","timeFrom":"511.917999","timeTo":"725.314 ","number":"6","chaptername":"Retroflexion in stomach ","description":" ","tagid":"369","tagName":"Assessment of the gastro-oesophageal junction"},{"id":"276","split":"1","chapterid":"793","timeFrom":"511.917999","timeTo":"725.314 ","number":"6","chaptername":"Retroflexion in stomach ","description":" ","tagid":"366","tagName":"Gastroscope handling"},{"id":"276","split":"1","chapterid":"794","timeFrom":"725.314999","timeTo":"1022.501 ","number":"7","chaptername":"Second inspection of oesophagus ","description":" ","tagid":"374","tagName":"Oesophageal lesions, inflammatory"},{"id":"276","split":"1","chapterid":"794","timeFrom":"725.314999","timeTo":"1022.501 ","number":"7","chaptername":"Second inspection of oesophagus ","description":" ","tagid":"370","tagName":"Benefit of simethicone"},{"id":"276","split":"1","chapterid":"794","timeFrom":"725.314999","timeTo":"1022.501 ","number":"7","chaptername":"Second inspection of oesophagus ","description":" ","tagid":"306","tagName":"Virtual chromoendoscopy"},{"id":"276","split":"1","chapterid":"794","timeFrom":"725.314999","timeTo":"1022.501 ","number":"7","chaptername":"Second inspection of oesophagus ","description":" ","tagid":"498","tagName":"LA classification of reflux oesophagitis"},{"id":"276","split":"1","chapterid":"794","timeFrom":"725.314999","timeTo":"1022.501 ","number":"7","chaptername":"Second inspection of oesophagus ","description":" ","tagid":"656","tagName":"Blue Light Imaging (BLI)"},{"id":"276","split":"1","chapterid":"796","timeFrom":"1440.69 ","timeTo":"1947.216 ","number":"9","chaptername":"Second live endoscopy: \"Lesion Characterisation at Upper GI\" ","description":" ","tagid":"370","tagName":"Benefit of simethicone"},{"id":"276","split":"1","chapterid":"796","timeFrom":"1440.69 ","timeTo":"1947.216 ","number":"9","chaptername":"Second live endoscopy: \"Lesion Characterisation at Upper GI\" ","description":" ","tagid":"442","tagName":"Desufflation"},{"id":"276","split":"1","chapterid":"796","timeFrom":"1440.69 ","timeTo":"1947.216 ","number":"9","chaptername":"Second live endoscopy: \"Lesion Characterisation at Upper GI\" ","description":" ","tagid":"654","tagName":"High Definition White Light (HDWL)"},{"id":"276","split":"1","chapterid":"796","timeFrom":"1440.69 ","timeTo":"1947.216 ","number":"9","chaptername":"Second live endoscopy: \"Lesion Characterisation at Upper GI\" ","description":" ","tagid":"493","tagName":"Targeted biopsies"},{"id":"276","split":"1","chapterid":"797","timeFrom":"1947.21699","timeTo":"2242.549 ","number":"10","chaptername":"Surprising detection of neoplastic lesion ","description":" ","tagid":"489","tagName":"Demarcated Area"},{"id":"276","split":"1","chapterid":"797","timeFrom":"1947.21699","timeTo":"2242.549 ","number":"10","chaptername":"Surprising detection of neoplastic lesion ","description":" ","tagid":"657","tagName":"Linked Colour Imaging (LCI)"},{"id":"276","split":"1","chapterid":"797","timeFrom":"1947.21699","timeTo":"2242.549 ","number":"10","chaptername":"Surprising detection of neoplastic lesion ","description":" ","tagid":"306","tagName":"Virtual chromoendoscopy"}]
[{"name":"Enhancing Gastroscopy Quality Through Advanced Techniques and Meticulous Examination","description":"The discussion emphasized meticulous gastroscopy, advanced imaging, targeted biopsies, completeness, and potential quality indicators to improve lesion detection and patient care.","summary":"
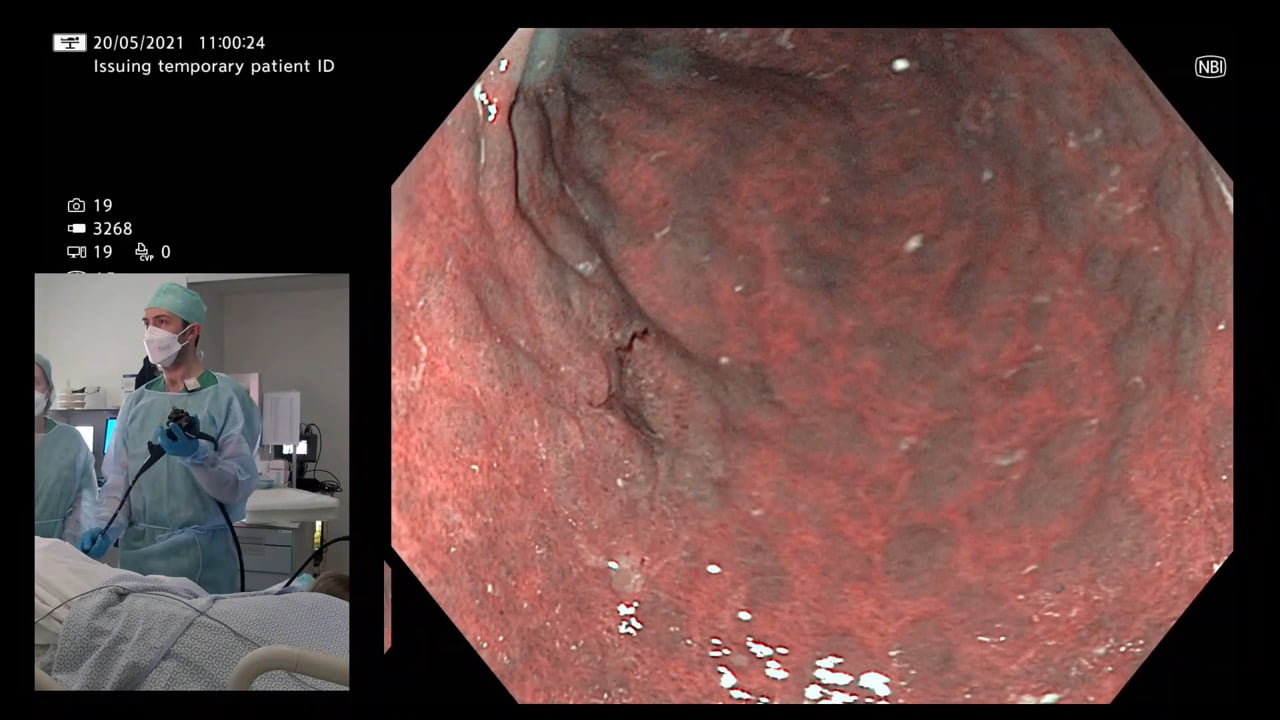
The medical symposium discussion revolved around the meticulous and comprehensive approach to gastroscopy, particularly in high-risk patients. Key points included the importance of dedicating ample time to the procedure, focusing on patient preparation, and utilizing advanced imaging techniques like narrow-band imaging (NBI), blue light imaging (BLI), and virtual chromoendoscopy for enhanced lesion detection. Targeted biopsies were recommended for suspicious areas, emphasizing the significance of quality over quantity when it comes to biopsying. The presence of an inlet patch in the upper esophagus was discussed as an area that may warrant biopsy if there are notable irregularities. Ensuring the completeness of the examination was stressed, not only for patient care but also for legal reasons. Visualizing the Papilla of Vater during gastroscopy emerged as a potential quality indicator. In essence, the discussion underscored the need for a systematic and thorough gastroscopy approach, highlighting the value of advanced techniques, targeted biopsies, and a holistic examination to improve lesion detection and patient outcomes while emphasizing the importance of continuous research to refine best practices in gastroscopy.<\/p>","detailedSummary":"
Learning Objectives:\u00e2\u0080\u00af <\/p>\n
\n
Emphasize the importance of meticulous gastroscopy.<\/li>\n
Utilize advanced imaging techniques for improved lesion detection.<\/li>\n
Target biopsies based on suspicious findings.<\/li>\n
Recognize the significance of completeness in endoscopic examinations.<\/li>\n
Consider potential quality indicators to enhance patient care and outcomes.<\/li>\n<\/ul>","author":"Triana Lobaton","tagger":"14","editor":"15","recorder":"13","authorid":"55","centreName":"Triana Lobaton","centreCity":"Ghent","centreCountry":"Belgium"}]
[{"chapterTagid":"2528","tagName":"Assessment of the gastro-oesophageal junction","id":"369"},{"chapterTagid":"2531","tagName":"Benefit of simethicone","id":"370"},{"chapterTagid":"2553","tagName":"Blue Light Imaging (BLI)","id":"656"},{"chapterTagid":"2555","tagName":"Demarcated Area","id":"489"},{"chapterTagid":"2541","tagName":"Describing position within the stomach","id":"497"},{"chapterTagid":"2551","tagName":"Desufflation","id":"442"},{"chapterTagid":"2534","tagName":"Duodenum","id":"262"},{"chapterTagid":"2533","tagName":"Gastroscope handling","id":"366"},{"chapterTagid":"2488","tagName":"GIEQs Digital Edition I","id":"569"},{"chapterTagid":"2552","tagName":"High Definition White Light (HDWL)","id":"654"},{"chapterTagid":"2539","tagName":"Hill Classification","id":"499"},{"chapterTagid":"2549","tagName":"LA classification of reflux oesophagitis","id":"498"},{"chapterTagid":"2557","tagName":"Linked Colour Imaging (LCI)","id":"657"},{"chapterTagid":"2546","tagName":"Oesophageal lesions, inflammatory","id":"374"},{"chapterTagid":"2536","tagName":"Oesophagus","id":"260"},{"chapterTagid":"2538","tagName":"Retroflexion in the stomach (J manouevre)","id":"500"},{"chapterTagid":"2535","tagName":"Stomach","id":"261"},{"chapterTagid":"2554","tagName":"Targeted biopsies","id":"493"},{"chapterTagid":"2529","tagName":"Tip attachments","id":"174"},{"chapterTagid":"2542","tagName":"Virtual chromoendoscopy","id":"306"},{"chapterTagid":"2532","tagName":"Visualisation of posterior wall of D2 and junction","id":"368"},{"chapterTagid":"2537","tagName":"Visualisation of the major papilla","id":"367"}]
The medical symposium discussion revolved around the meticulous and comprehensive approach to gastroscopy, particularly in high-risk patients. Key points included the importance of dedicating ample time to the procedure, focusing on patient preparation, and utilizing advanced imaging techniques like narrow-band imaging (NBI), blue light imaging (BLI), and virtual chromoendoscopy for enhanced lesion detection. Targeted biopsies were recommended for suspicious areas, emphasizing the significance of quality over quantity when it comes to biopsying. The presence of an inlet patch in the upper esophagus was discussed as an area that may warrant biopsy if there are notable irregularities. Ensuring the completeness of the examination was stressed, not only for patient care but also for legal reasons. Visualizing the Papilla of Vater during gastroscopy emerged as a potential quality indicator. In essence, the discussion underscored the need for a systematic and thorough gastroscopy approach, highlighting the value of advanced techniques, targeted biopsies, and a holistic examination to improve lesion detection and patient outcomes while emphasizing the importance of continuous research to refine best practices in gastroscopy.
Detailed Summary
Learning Objectives:â¯
Emphasize the importance of meticulous gastroscopy.
Utilize advanced imaging techniques for improved lesion detection.
Target biopsies based on suspicious findings.
Recognize the significance of completeness in endoscopic examinations.
Consider potential quality indicators to enhance patient care and outcomes.
Assessment of the gastro-oesophageal junctionBenefit of simethiconeGastroscope handlingRetroflexion in the stomach (J manouevre)Visualisation of posterior wall of D2 and junctionVisualisation of the major papilla
GIEQs Digital Edition I
GIEQs Digital Edition I
Imaging modalities
Virtual chromoendoscopy
Other techniques
Desufflation
Techniques in diagnostic gastroscopy
Describing position within the stomach
Upper GI Classifications
Hill ClassificationLA classification of reflux oesophagitis
Upper GI diagnostic techniques
Targeted biopsies
Upper GI Image Enhancement
Blue Light Imaging (BLI)High Definition White Light (HDWL)Linked Colour Imaging (LCI)
Registration will open in late January 2020. Prior to this you
can register your interest below and we will keep you updated on everything GIEQs.Your email address will only be used to update you on GIEQs
Join us for GIEQs II
Released prior to the early bird deadline these 6, 1-2 minute video
snippets
demonstrate the attention to detail, deconstructed approach and rock solid evidence
base of the GIEQs Approach.
1 - Over the Scope Clip for Upper
Gastrointestinal Bleeding Use of
OTSC as first-line for life
threatening upper gastrointestinal haemorrhage.
2 - Early Gastric Cancer Can you
identify and characterise
this early gastric cancer? Watch the video for more information
including endoscopic resectability
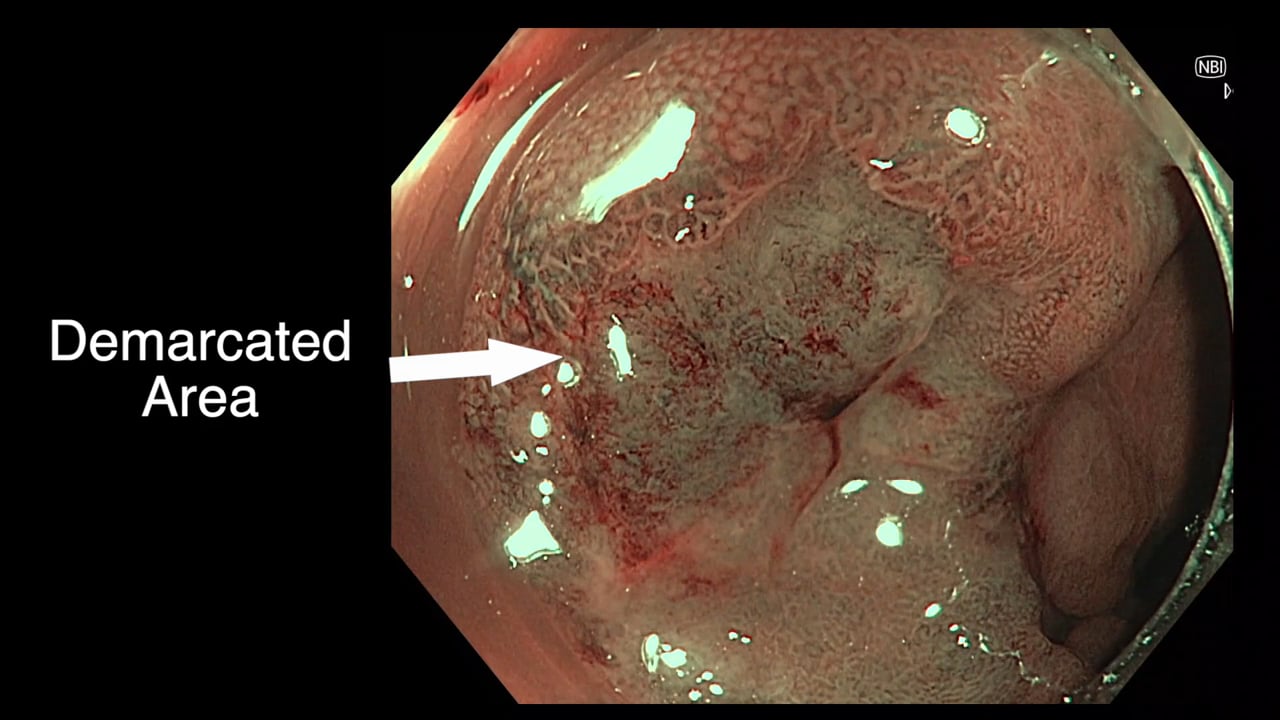
3 - The Demarcated Area as a Predictor of
Submucosal Invasion in Colon Polyps the Demarcated Area has emerged as a stable predictor
of submucosal invasive cancer. Find out more here.
4 - Dealing with Adverse Events at Colonic
Polypectomy
To be able to competently perform colonic polypectomy you must be able
to deal with adverse events. A deconstructed example is shown
here.
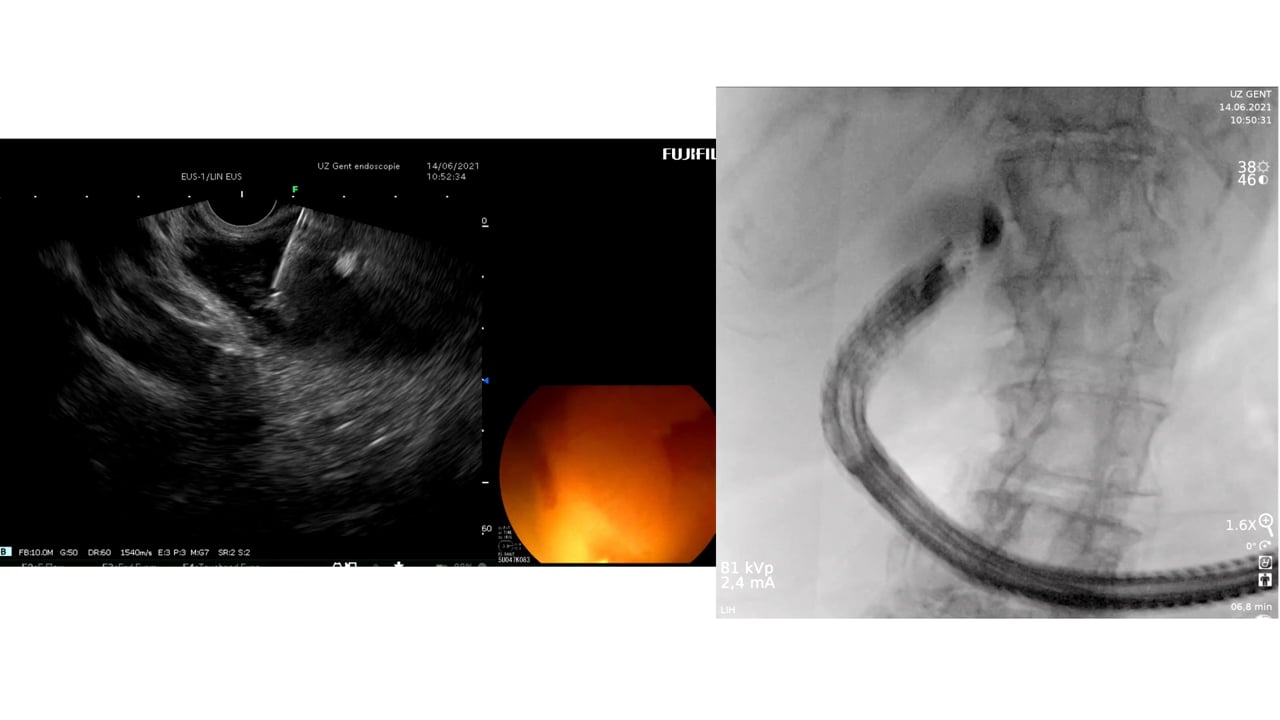
5 - Complex EUS applications to make Everyday
ERCP easier Endoscopic Ultrasound
is radically changing the way we approach biliary intervention and can
make a difference to everyday endoscopic problems.
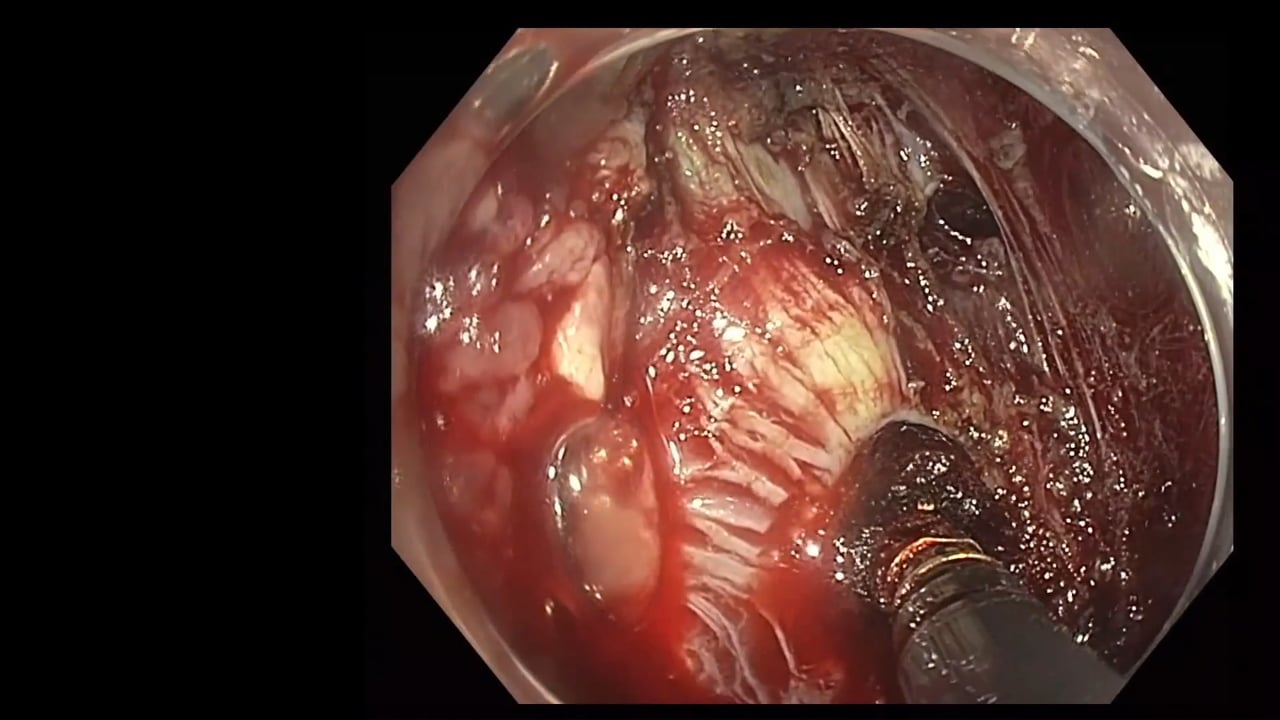
6 - Decision Making after Large perforation and
life threatening Bleeding during Polypectomy Many of the GIEQs faculty spend their normal working
lives on complex endoscopy. Learning the lessons and approach from these
procedures, deconstructing them and bringing them to the everyday is a
crucial part of the GIEQs approach.