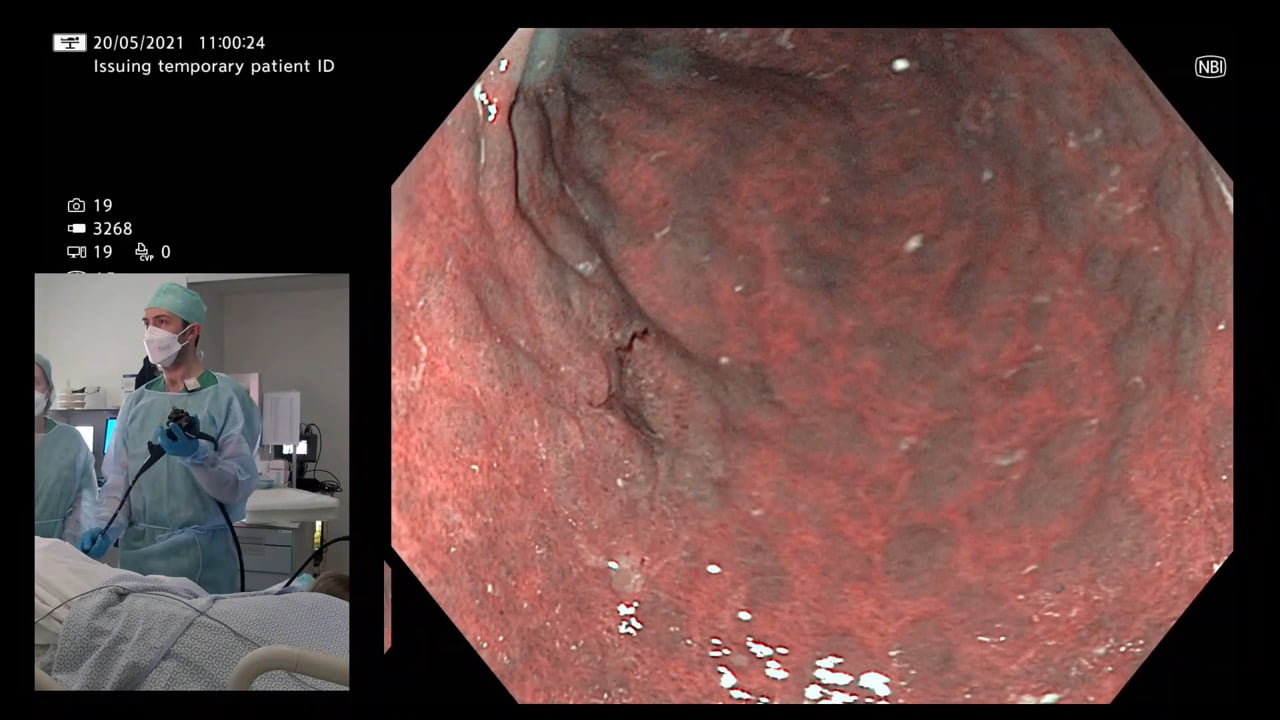
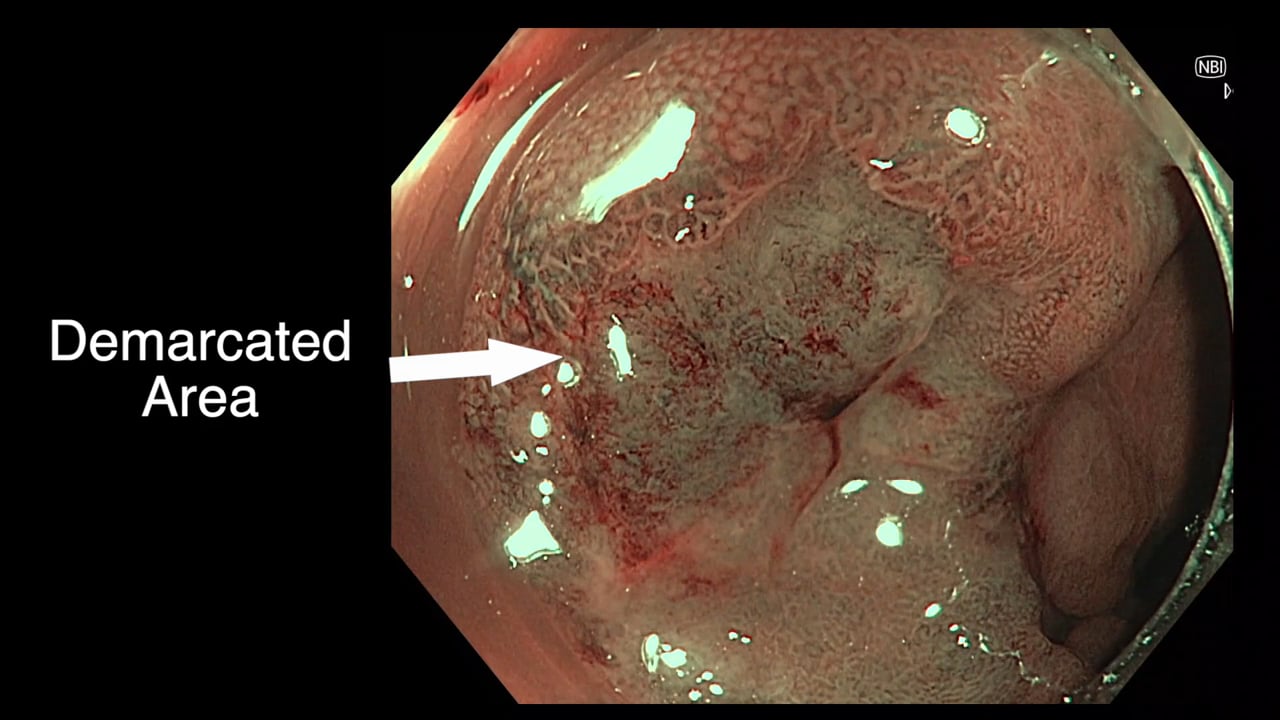
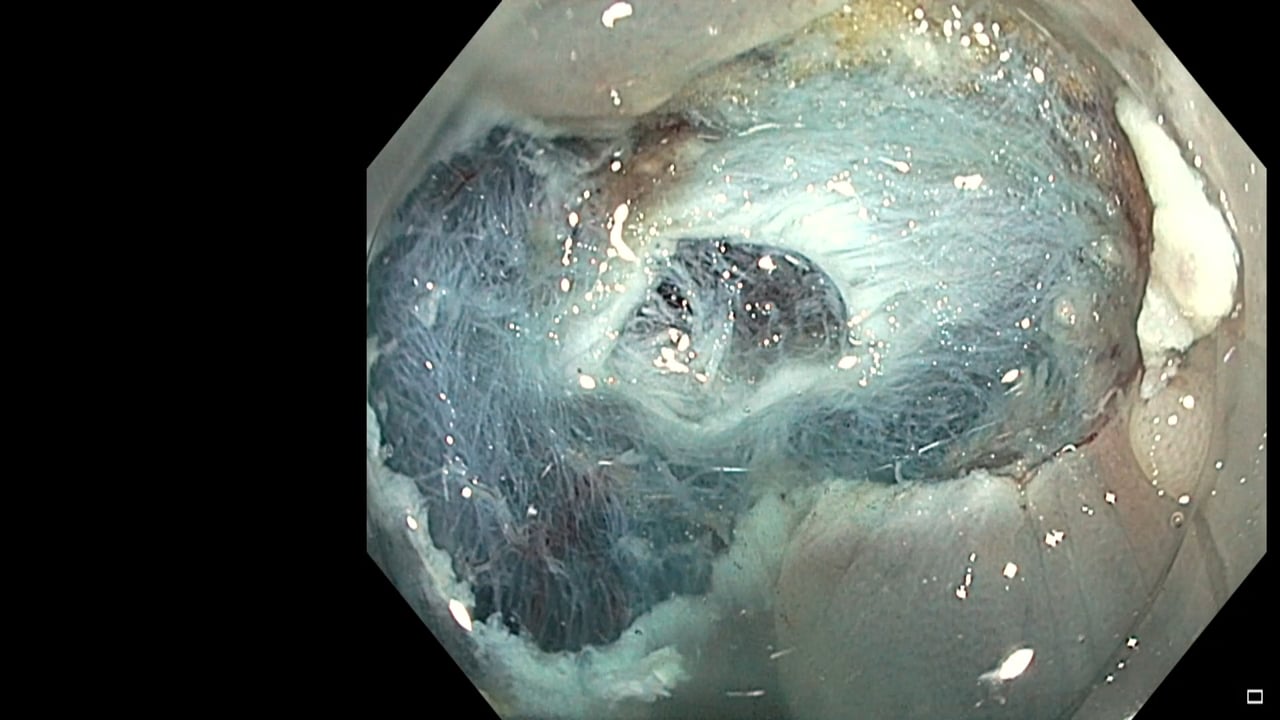
[{"id":"157","chapterid":"520","timeTo":"30 ","timeFrom":"0 ","number":"1","chaptername":"Lesion assessment ","description":"Assessment from afar\n- not homogenous\n- Paris 0-Is\n- non-granular "},{"id":"157","chapterid":"522","timeTo":"78.883 ","timeFrom":"30.001 ","number":"2","chaptername":"Magnification ","description":"Regular surrounding Kudo type IV pattern\n- Demarcated area within with some areas of Kudo Vn pattern "},{"id":"157","chapterid":"523","timeTo":"160.343 ","timeFrom":"78.884 ","number":"3","chaptername":"Discussion of treatment options ","description":"This deeply invasive lesion should be removed using surgical resection with lymph node clearance "},{"id":"157","chapterid":"524","timeTo":"197.195 ","timeFrom":"160.344 ","number":"4","chaptername":"Description of the position of the lesion ","description":"To describe the position of a lesion in the ascending colon use the ileo-caecal valve as medial and describe in number of folds distal and use the positions superior, inferior, medial and lateral. This lesion is clearly medial and 2 folds back from the ICV "},{"id":"157","chapterid":"525","timeTo":"263.684 ","timeFrom":"197.196 ","number":"5","chaptername":"Biopsying a malignancy ","description":"Biopsy the area of most disordered pit pattern. Take one biopsy only at a time if you are trying to biopsy something specific. "},{"id":"157","chapterid":"526","timeTo":"275.248 ","timeFrom":"263.685 ","number":"6","chaptername":"Tethered lesion ","description":"Lesion moves as one whilst attached to the instrument suggesting deep submucosal tethering "},{"id":"157","chapterid":"527","timeTo":"453.781 ","timeFrom":"275.248999","number":"7","chaptername":"Placing an Indian Ink Mark ","description":"Technique includes\n- not marking around other lesions\n- marking distal\n- avoiding caecum and rectum\n- saline injection first and switch to tattoo to avoid transmural injection\n- two marks at least on opposite sides of the colonic lumen "}]
[{"id":"157","split":"1","chapterid":"520","timeFrom":"0 ","timeTo":"30 ","number":"1","chaptername":"Lesion assessment ","description":"Assessment from afar\n- not homogenous\n- Paris 0-Is\n- non-granular ","tagid":"256","tagName":"Endoscopic Video and Audio Narration"},{"id":"157","split":"1","chapterid":"520","timeFrom":"0 ","timeTo":"30 ","number":"1","chaptername":"Lesion assessment ","description":"Assessment from afar\n- not homogenous\n- Paris 0-Is\n- non-granular ","tagid":"309","tagName":"Non-granular"},{"id":"157","split":"1","chapterid":"520","timeFrom":"0 ","timeTo":"30 ","number":"1","chaptername":"Lesion assessment ","description":"Assessment from afar\n- not homogenous\n- Paris 0-Is\n- non-granular ","tagid":"314","tagName":"NICE III"},{"id":"157","split":"1","chapterid":"520","timeFrom":"0 ","timeTo":"30 ","number":"1","chaptername":"Lesion assessment ","description":"Assessment from afar\n- not homogenous\n- Paris 0-Is\n- non-granular ","tagid":"325","tagName":"Paris 0-Is"},{"id":"157","split":"1","chapterid":"522","timeFrom":"30.001 ","timeTo":"78.883 ","number":"2","chaptername":"Magnification ","description":"Regular surrounding Kudo type IV pattern\n- Demarcated area within with some areas of Kudo Vn pattern ","tagid":"449","tagName":"[high risk] Demarcated area of disordered pit\/vascular pattern"},{"id":"157","split":"1","chapterid":"522","timeFrom":"30.001 ","timeTo":"78.883 ","number":"2","chaptername":"Magnification ","description":"Regular surrounding Kudo type IV pattern\n- Demarcated area within with some areas of Kudo Vn pattern ","tagid":"320","tagName":"Kudo Vn"},{"id":"157","split":"1","chapterid":"523","timeFrom":"78.884 ","timeTo":"160.343 ","number":"3","chaptername":"Discussion of treatment options ","description":"This deeply invasive lesion should be removed using surgical resection with lymph node clearance ","tagid":"473","tagName":"Whether to biopsy a suspicious polyp"},{"id":"157","split":"1","chapterid":"523","timeFrom":"78.884 ","timeTo":"160.343 ","number":"3","chaptername":"Discussion of treatment options ","description":"This deeply invasive lesion should be removed using surgical resection with lymph node clearance ","tagid":"472","tagName":"Endoscopic versus Surgical Management"},{"id":"157","split":"1","chapterid":"525","timeFrom":"197.196 ","timeTo":"263.684 ","number":"5","chaptername":"Biopsying a malignancy ","description":"Biopsy the area of most disordered pit pattern. Take one biopsy only at a time if you are trying to biopsy something specific. ","tagid":"473","tagName":"Whether to biopsy a suspicious polyp"},{"id":"157","split":"1","chapterid":"526","timeFrom":"263.685 ","timeTo":"275.248 ","number":"6","chaptername":"Tethered lesion ","description":"Lesion moves as one whilst attached to the instrument suggesting deep submucosal tethering ","tagid":"567","tagName":"[high risk] Lesion moves as one, indicating deep tethering"},{"id":"157","split":"1","chapterid":"527","timeFrom":"275.248999","timeTo":"453.781 ","number":"7","chaptername":"Placing an Indian Ink Mark ","description":"Technique includes\n- not marking around other lesions\n- marking distal\n- avoiding caecum and rectum\n- saline injection first and switch to tattoo to avoid transmural injection\n- two marks at least on opposite sides of the colonic lumen ","tagid":"474","tagName":"Tattoo placement"}]
[{"name":"Malignant polyp in the ascending colon","description":"Endoscopic evaluation and further management of a malignant polyp in the ascending colon. Covers imaging, where to biopsy and spot marking","summary":"","detailedSummary":"","author":"David Tate","tagger":"1","editor":"9","recorder":"9","authorid":"1","centreName":"University Hospital of Ghent","centreCity":"Ghent","centreCountry":"Belgium"}]
[{"chapterTagid":"1575","tagName":"Endoscopic versus Surgical Management","id":"472"},{"chapterTagid":"1554","tagName":"Endoscopic Video and Audio Narration","id":"256"},{"chapterTagid":"1573","tagName":"Kudo Vn","id":"320"},{"chapterTagid":"1570","tagName":"NICE III","id":"314"},{"chapterTagid":"1569","tagName":"Non-granular","id":"309"},{"chapterTagid":"1571","tagName":"Paris 0-Is","id":"325"},{"chapterTagid":"1582","tagName":"Tattoo placement","id":"474"},{"chapterTagid":"1574","tagName":"Whether to biopsy a suspicious polyp","id":"473"},{"chapterTagid":"1572","tagName":"[high risk] Demarcated area of disordered pit\/vascular pattern","id":"449"},{"chapterTagid":"1583","tagName":"[high risk] Lesion moves as one, indicating deep tethering","id":"567"}]
Registration will open in late January 2020. Prior to this you
can register your interest below and we will keep you updated on everything GIEQs.Your email address will only be used to update you on GIEQs
Join us for GIEQs II
Released prior to the early bird deadline these 6, 1-2 minute video
snippets
demonstrate the attention to detail, deconstructed approach and rock solid evidence
base of the GIEQs Approach.
1 - Over the Scope Clip for Upper
Gastrointestinal Bleeding Use of
OTSC as first-line for life
threatening upper gastrointestinal haemorrhage.
2 - Early Gastric Cancer Can you
identify and characterise
this early gastric cancer? Watch the video for more information
including endoscopic resectability
3 - The Demarcated Area as a Predictor of
Submucosal Invasion in Colon Polyps the Demarcated Area has emerged as a stable predictor
of submucosal invasive cancer. Find out more here.
4 - Dealing with Adverse Events at Colonic
Polypectomy
To be able to competently perform colonic polypectomy you must be able
to deal with adverse events. A deconstructed example is shown
here.
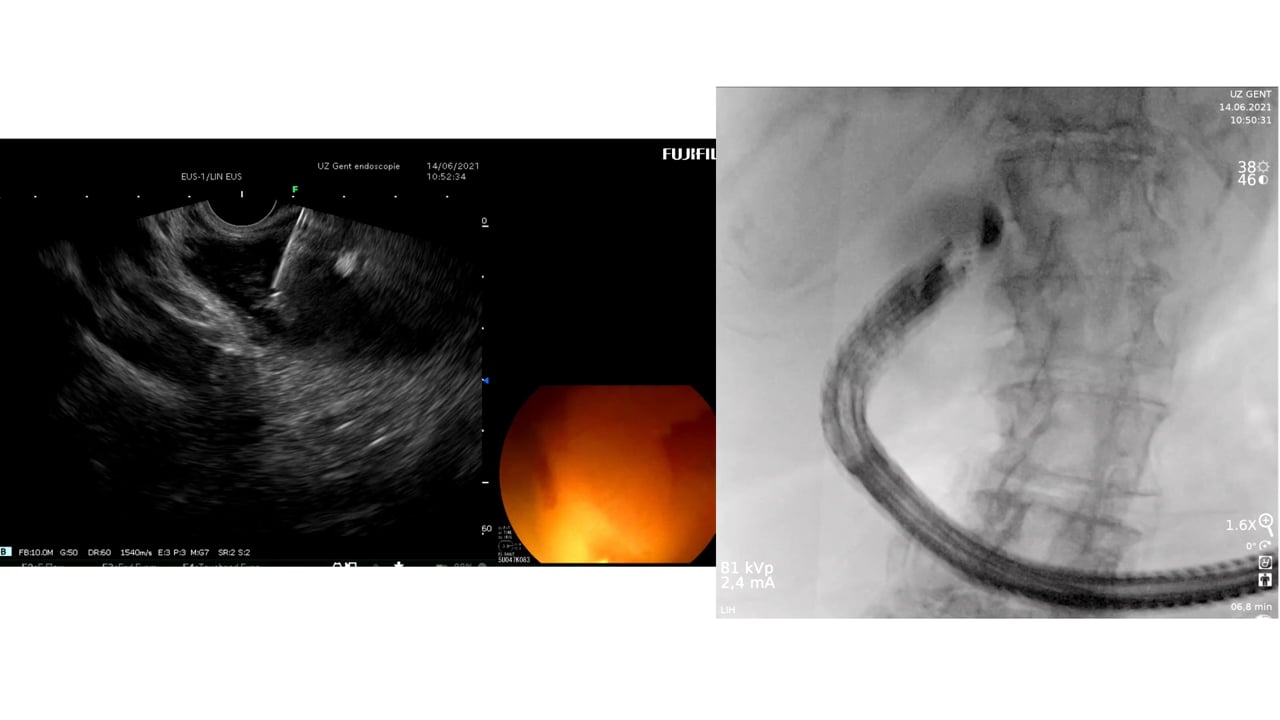
5 - Complex EUS applications to make Everyday
ERCP easier Endoscopic Ultrasound
is radically changing the way we approach biliary intervention and can
make a difference to everyday endoscopic problems.
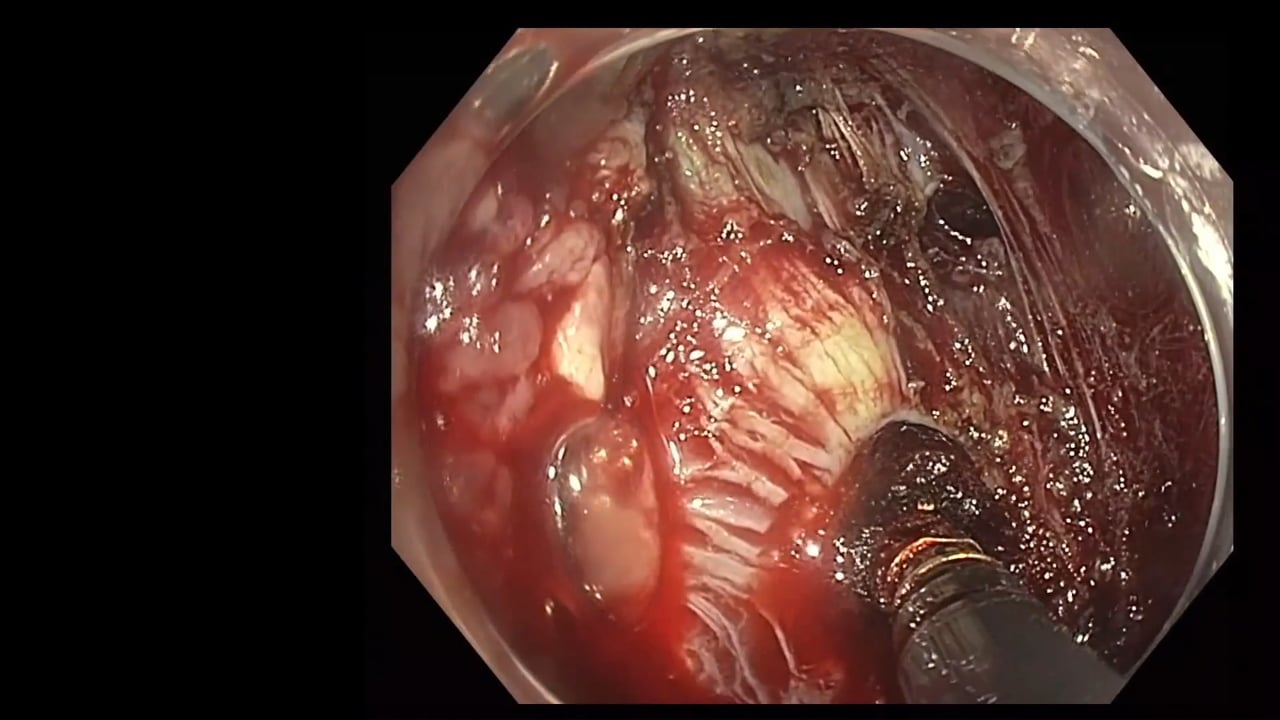
6 - Decision Making after Large perforation and
life threatening Bleeding during Polypectomy Many of the GIEQs faculty spend their normal working
lives on complex endoscopy. Learning the lessons and approach from these
procedures, deconstructing them and bringing them to the everyday is a
crucial part of the GIEQs approach.