[{"id":"113","chapterid":"201","timeTo":"105.431 ","timeFrom":"4.475 ","number":"1","chaptername":"Lesion assessment ","description":"Description of a laterally spreading lesion with overall assessment, Paris classification, morphology. Virtual chromoendoscopy is demonstrated.\n\nThe lesion has a Kudo IIIS\/L, NICE II pit\/vascular pattern using virtual chromoendoscopy. It is of Paris 0-IIa morphology. "},{"id":"113","chapterid":"202","timeTo":"171.615 ","timeFrom":"105.432 ","number":"2","chaptername":"Choice of resection technique ","description":"The discussion centres around the risk of submucosal invasion versus the risks and invasiveness of the technique. "},{"id":"113","chapterid":"203","timeTo":"220.178 ","timeFrom":"171.616 ","number":"3","chaptername":"Choice of snare ","description":"Discussion of the type of snare required for this lesion.\nIf a decision has been made to perform hot snare polypectomy a hot snare (thicker wire, here 0.47mm) should be used "},{"id":"113","chapterid":"204","timeTo":"300.758 ","timeFrom":"220.179 ","number":"4","chaptername":"Injection technique ","description":"The technique of dynamic injection is demonstrated\n- using the needle to make a stab and immediately withdrawing to find the submucosal plane. Once the plane is found the lesion will immediately start to lift. Once lifting begins the lesion can be moved in any direction to make access to the lesion easier thereafter. "},{"id":"113","chapterid":"205","timeTo":"355.761 ","timeFrom":"300.758999","number":"5","chaptername":"Choice of polypectomy technique ","description":"Further discussion of choice of technique and snare type.\nThe snare used here is an Olympus SnareMaster 15mm snare. "},{"id":"113","chapterid":"206","timeTo":"428.385 ","timeFrom":"355.762 ","number":"6","chaptername":"Snare placement technique ","description":"Discussion points\n- opening the snare and then controlling it yourself adds control\n- placement with a wide margin of normal tissue is optimal\n- closure onto a fold results in the appearances here "},{"id":"113","chapterid":"207","timeTo":"478.326 ","timeFrom":"428.385999","number":"7","chaptername":"Safety checks before applying diathermy ","description":"Safety checks before application of diathermy\n- visualise specimen\n- ensure free movement from underlying colonic structures\n- ensure feel of tissue is spongy\n- ensure correct generator settings "},{"id":"113","chapterid":"208","timeTo":"568.641 ","timeFrom":"478.327 ","number":"8","chaptername":"Defect assesssment during resection ","description":"The techniques of inject and resect EMR are discussed "},{"id":"113","chapterid":"209","timeTo":"601.626 ","timeFrom":"568.641 ","number":"9","chaptername":"Optimal snare placement ","description":"The techniques of inject and resect EMR are discussed "},{"id":"113","chapterid":"210","timeTo":"628.724 ","timeFrom":"601.627 ","number":"10","chaptername":"Safety checks before applying diathermy ","description":"Safety checks before application of diathermy\n- visualise specimen\n- ensure free movement from underlying colonic structures\n- ensure feel of tissue is spongy\n- ensure correct generator settings "},{"id":"113","chapterid":"211","timeTo":"755.365 ","timeFrom":"628.725 ","number":"11","chaptername":"Injection technique ","description":"The techniques of inject and resect EMR are discussed "},{"id":"113","chapterid":"212","timeTo":"834.13 ","timeFrom":"755.366 ","number":"12","chaptername":"Snare placement ","description":"The techniques of inject and resect EMR are discussed "},{"id":"113","chapterid":"213","timeTo":"866.163 ","timeFrom":"834.131 ","number":"13","chaptername":"Safety checks before applying diathermy ","description":"Safety checks before application of diathermy\n- visualise specimen\n- ensure free movement from underlying colonic structures\n- ensure feel of tissue is spongy\n- ensure correct generator settings "},{"id":"113","chapterid":"214","timeTo":"929.051 ","timeFrom":"866.164 ","number":"14","chaptername":"Assessment of the post-polypectomy defect ","description":"Injection with the tip of the injection catheter (without the needle - blunt injection) is used to assess for safety (evidence of deep mural injury) and for expanding the submucosal plane for the next resection "},{"id":"113","chapterid":"215","timeTo":"1060.649 ","timeFrom":"929.052 ","number":"15","chaptername":"Defect inspection after EMR ","description":"Features of the post-EMR resection defect are demonstrated and discussed\n- submucosal blood vessels\n- submucosal adipose tissue\n\nThe potential for clip closure of the defect is discussed along with reasons for and against "},{"id":"113","chapterid":"216","timeTo":"1265.984 ","timeFrom":"1060.64999","number":"16","chaptername":"Technique for thermal ablation of the post EMR margin ","description":"The technique for margin ablation involves\n- keeping the catheter still\n- perfecting your tip control\n- creating a 1mm rim of ablated tissue around the full circumference of the lesion\n\n- recent data suggests that incomplete margin ablation removes the protective effect of the technique at surveillance endoscopy "},{"id":"113","chapterid":"217","timeTo":"1389.592 ","timeFrom":"1265.985 ","number":"17","chaptername":"Technique for clip closure of the post-EMR defect ","description":"No deep injury is demonstrated within this defect (DMI type 0). The clip closure is for risk of bleeding (proximal colonic lesion).\n\nThe technique for clip closure is discussed\n- planning, (difficult to easy, left to right)\n- placement\n- rotation\n- suction and closure "},{"id":"113","chapterid":"218","timeTo":"1500.373 ","timeFrom":"1389.593 ","number":"18","chaptername":"Feedback on performance ","description":"Done well\n- tip control, margin ablation\n\n\nCould improve\n- lesion assessment\n- lifting, stab and pull back\n- avoid capture of tissue over folds\n- placement of clips "}]
[{"id":"113","split":"1","chapterid":"201","timeFrom":"4.475 ","timeTo":"105.431 ","number":"1","chaptername":"Lesion assessment ","description":"Description of a laterally spreading lesion with overall assessment, Paris classification, morphology. Virtual chromoendoscopy is demonstrated.\n\nThe lesion has a Kudo IIIS\/L, NICE II pit\/vascular pattern using virtual chromoendoscopy. It is of Paris 0-IIa morphology. ","tagid":"306","tagName":"Virtual chromoendoscopy"},{"id":"113","split":"1","chapterid":"201","timeFrom":"4.475 ","timeTo":"105.431 ","number":"1","chaptername":"Lesion assessment ","description":"Description of a laterally spreading lesion with overall assessment, Paris classification, morphology. Virtual chromoendoscopy is demonstrated.\n\nThe lesion has a Kudo IIIS\/L, NICE II pit\/vascular pattern using virtual chromoendoscopy. It is of Paris 0-IIa morphology. ","tagid":"302","tagName":"Kudo Classification"},{"id":"113","split":"1","chapterid":"201","timeFrom":"4.475 ","timeTo":"105.431 ","number":"1","chaptername":"Lesion assessment ","description":"Description of a laterally spreading lesion with overall assessment, Paris classification, morphology. Virtual chromoendoscopy is demonstrated.\n\nThe lesion has a Kudo IIIS\/L, NICE II pit\/vascular pattern using virtual chromoendoscopy. It is of Paris 0-IIa morphology. ","tagid":"301","tagName":"NICE classification"},{"id":"113","split":"1","chapterid":"201","timeFrom":"4.475 ","timeTo":"105.431 ","number":"1","chaptername":"Lesion assessment ","description":"Description of a laterally spreading lesion with overall assessment, Paris classification, morphology. Virtual chromoendoscopy is demonstrated.\n\nThe lesion has a Kudo IIIS\/L, NICE II pit\/vascular pattern using virtual chromoendoscopy. It is of Paris 0-IIa morphology. ","tagid":"323","tagName":"Paris 0-IIa"},{"id":"113","split":"1","chapterid":"201","timeFrom":"4.475 ","timeTo":"105.431 ","number":"1","chaptername":"Lesion assessment ","description":"Description of a laterally spreading lesion with overall assessment, Paris classification, morphology. Virtual chromoendoscopy is demonstrated.\n\nThe lesion has a Kudo IIIS\/L, NICE II pit\/vascular pattern using virtual chromoendoscopy. It is of Paris 0-IIa morphology. ","tagid":"264","tagName":"Colon"},{"id":"113","split":"1","chapterid":"201","timeFrom":"4.475 ","timeTo":"105.431 ","number":"1","chaptername":"Lesion assessment ","description":"Description of a laterally spreading lesion with overall assessment, Paris classification, morphology. Virtual chromoendoscopy is demonstrated.\n\nThe lesion has a Kudo IIIS\/L, NICE II pit\/vascular pattern using virtual chromoendoscopy. It is of Paris 0-IIa morphology. ","tagid":"309","tagName":"Non-granular"},{"id":"113","split":"1","chapterid":"201","timeFrom":"4.475 ","timeTo":"105.431 ","number":"1","chaptername":"Lesion assessment ","description":"Description of a laterally spreading lesion with overall assessment, Paris classification, morphology. Virtual chromoendoscopy is demonstrated.\n\nThe lesion has a Kudo IIIS\/L, NICE II pit\/vascular pattern using virtual chromoendoscopy. It is of Paris 0-IIa morphology. ","tagid":"462","tagName":"Endoscopic Video and Room Video with Audio Plus Trainee"},{"id":"113","split":"1","chapterid":"202","timeFrom":"105.432 ","timeTo":"171.615 ","number":"2","chaptername":"Choice of resection technique ","description":"The discussion centres around the risk of submucosal invasion versus the risks and invasiveness of the technique. ","tagid":"294","tagName":"Endoscopic Mucosal Resection (piecemeal)"},{"id":"113","split":"1","chapterid":"202","timeFrom":"105.432 ","timeTo":"171.615 ","number":"2","chaptername":"Choice of resection technique ","description":"The discussion centres around the risk of submucosal invasion versus the risks and invasiveness of the technique. ","tagid":"445","tagName":"En bloc versus piecemeal resection"},{"id":"113","split":"1","chapterid":"202","timeFrom":"105.432 ","timeTo":"171.615 ","number":"2","chaptername":"Choice of resection technique ","description":"The discussion centres around the risk of submucosal invasion versus the risks and invasiveness of the technique. ","tagid":"447","tagName":"[low risk] Right colon, flat, no nodules"},{"id":"113","split":"1","chapterid":"203","timeFrom":"171.616 ","timeTo":"220.178 ","number":"3","chaptername":"Choice of snare ","description":"Discussion of the type of snare required for this lesion.\nIf a decision has been made to perform hot snare polypectomy a hot snare (thicker wire, here 0.47mm) should be used ","tagid":"289","tagName":"Large (20mm or larger)"},{"id":"113","split":"1","chapterid":"203","timeFrom":"171.616 ","timeTo":"220.178 ","number":"3","chaptername":"Choice of snare ","description":"Discussion of the type of snare required for this lesion.\nIf a decision has been made to perform hot snare polypectomy a hot snare (thicker wire, here 0.47mm) should be used ","tagid":"444","tagName":"Choice of snare type"},{"id":"113","split":"1","chapterid":"203","timeFrom":"171.616 ","timeTo":"220.178 ","number":"3","chaptername":"Choice of snare ","description":"Discussion of the type of snare required for this lesion.\nIf a decision has been made to perform hot snare polypectomy a hot snare (thicker wire, here 0.47mm) should be used ","tagid":"446","tagName":"Hot versus cold snare polypectomy"},{"id":"113","split":"1","chapterid":"204","timeFrom":"220.179 ","timeTo":"300.758 ","number":"4","chaptername":"Injection technique ","description":"The technique of dynamic injection is demonstrated\n- using the needle to make a stab and immediately withdrawing to find the submucosal plane. Once the plane is found the lesion will immediately start to lift. Once lifting begins the lesion can be moved in any direction to make access to the lesion easier thereafter. ","tagid":"269","tagName":"Injection technique"},{"id":"113","split":"1","chapterid":"205","timeFrom":"300.758999","timeTo":"355.761 ","number":"5","chaptername":"Choice of polypectomy technique ","description":"Further discussion of choice of technique and snare type.\nThe snare used here is an Olympus SnareMaster 15mm snare. ","tagid":"445","tagName":"En bloc versus piecemeal resection"},{"id":"113","split":"1","chapterid":"205","timeFrom":"300.758999","timeTo":"355.761 ","number":"5","chaptername":"Choice of polypectomy technique ","description":"Further discussion of choice of technique and snare type.\nThe snare used here is an Olympus SnareMaster 15mm snare. ","tagid":"444","tagName":"Choice of snare type"},{"id":"113","split":"1","chapterid":"206","timeFrom":"355.762 ","timeTo":"428.385 ","number":"6","chaptername":"Snare placement technique ","description":"Discussion points\n- opening the snare and then controlling it yourself adds control\n- placement with a wide margin of normal tissue is optimal\n- closure onto a fold results in the appearances here ","tagid":"270","tagName":"Snare placement"},{"id":"113","split":"1","chapterid":"207","timeFrom":"428.385999","timeTo":"478.326 ","number":"7","chaptername":"Safety checks before applying diathermy ","description":"Safety checks before application of diathermy\n- visualise specimen\n- ensure free movement from underlying colonic structures\n- ensure feel of tissue is spongy\n- ensure correct generator settings ","tagid":"271","tagName":"Safety checks prior to application of diathermy"},{"id":"113","split":"1","chapterid":"208","timeFrom":"478.327 ","timeTo":"568.641 ","number":"8","chaptername":"Defect assesssment during resection ","description":"The techniques of inject and resect EMR are discussed ","tagid":"272","tagName":"Post polypectomy defect assessment"},{"id":"113","split":"1","chapterid":"208","timeFrom":"478.327 ","timeTo":"568.641 ","number":"8","chaptername":"Defect assesssment during resection ","description":"The techniques of inject and resect EMR are discussed ","tagid":"269","tagName":"Injection technique"},{"id":"113","split":"1","chapterid":"209","timeFrom":"568.641 ","timeTo":"601.626 ","number":"9","chaptername":"Optimal snare placement ","description":"The techniques of inject and resect EMR are discussed ","tagid":"270","tagName":"Snare placement"},{"id":"113","split":"1","chapterid":"210","timeFrom":"601.627 ","timeTo":"628.724 ","number":"10","chaptername":"Safety checks before applying diathermy ","description":"Safety checks before application of diathermy\n- visualise specimen\n- ensure free movement from underlying colonic structures\n- ensure feel of tissue is spongy\n- ensure correct generator settings ","tagid":"271","tagName":"Safety checks prior to application of diathermy"},{"id":"113","split":"1","chapterid":"211","timeFrom":"628.725 ","timeTo":"755.365 ","number":"11","chaptername":"Injection technique ","description":"The techniques of inject and resect EMR are discussed ","tagid":"269","tagName":"Injection technique"},{"id":"113","split":"1","chapterid":"211","timeFrom":"628.725 ","timeTo":"755.365 ","number":"11","chaptername":"Injection technique ","description":"The techniques of inject and resect EMR are discussed ","tagid":"452","tagName":"Blunt injection"},{"id":"113","split":"1","chapterid":"211","timeFrom":"628.725 ","timeTo":"755.365 ","number":"11","chaptername":"Injection technique ","description":"The techniques of inject and resect EMR are discussed ","tagid":"454","tagName":"Stab and pull back to find submucosal plane"},{"id":"113","split":"1","chapterid":"211","timeFrom":"628.725 ","timeTo":"755.365 ","number":"11","chaptername":"Injection technique ","description":"The techniques of inject and resect EMR are discussed ","tagid":"453","tagName":"Dynamic injection"},{"id":"113","split":"1","chapterid":"212","timeFrom":"755.366 ","timeTo":"834.13 ","number":"12","chaptername":"Snare placement ","description":"The techniques of inject and resect EMR are discussed ","tagid":"270","tagName":"Snare placement"},{"id":"113","split":"1","chapterid":"213","timeFrom":"834.131 ","timeTo":"866.163 ","number":"13","chaptername":"Safety checks before applying diathermy ","description":"Safety checks before application of diathermy\n- visualise specimen\n- ensure free movement from underlying colonic structures\n- ensure feel of tissue is spongy\n- ensure correct generator settings ","tagid":"271","tagName":"Safety checks prior to application of diathermy"},{"id":"113","split":"1","chapterid":"214","timeFrom":"866.164 ","timeTo":"929.051 ","number":"14","chaptername":"Assessment of the post-polypectomy defect ","description":"Injection with the tip of the injection catheter (without the needle - blunt injection) is used to assess for safety (evidence of deep mural injury) and for expanding the submucosal plane for the next resection ","tagid":"272","tagName":"Post polypectomy defect assessment"},{"id":"113","split":"1","chapterid":"214","timeFrom":"866.164 ","timeTo":"929.051 ","number":"14","chaptername":"Assessment of the post-polypectomy defect ","description":"Injection with the tip of the injection catheter (without the needle - blunt injection) is used to assess for safety (evidence of deep mural injury) and for expanding the submucosal plane for the next resection ","tagid":"452","tagName":"Blunt injection"},{"id":"113","split":"1","chapterid":"215","timeFrom":"929.052 ","timeTo":"1060.649 ","number":"15","chaptername":"Defect inspection after EMR ","description":"Features of the post-EMR resection defect are demonstrated and discussed\n- submucosal blood vessels\n- submucosal adipose tissue\n\nThe potential for clip closure of the defect is discussed along with reasons for and against ","tagid":"272","tagName":"Post polypectomy defect assessment"},{"id":"113","split":"1","chapterid":"215","timeFrom":"929.052 ","timeTo":"1060.649 ","number":"15","chaptername":"Defect inspection after EMR ","description":"Features of the post-EMR resection defect are demonstrated and discussed\n- submucosal blood vessels\n- submucosal adipose tissue\n\nThe potential for clip closure of the defect is discussed along with reasons for and against ","tagid":"461","tagName":"Submucosal adipose tissue"},{"id":"113","split":"1","chapterid":"215","timeFrom":"929.052 ","timeTo":"1060.649 ","number":"15","chaptername":"Defect inspection after EMR ","description":"Features of the post-EMR resection defect are demonstrated and discussed\n- submucosal blood vessels\n- submucosal adipose tissue\n\nThe potential for clip closure of the defect is discussed along with reasons for and against ","tagid":"458","tagName":"Submucosal blood vessels"},{"id":"113","split":"1","chapterid":"215","timeFrom":"929.052 ","timeTo":"1060.649 ","number":"15","chaptername":"Defect inspection after EMR ","description":"Features of the post-EMR resection defect are demonstrated and discussed\n- submucosal blood vessels\n- submucosal adipose tissue\n\nThe potential for clip closure of the defect is discussed along with reasons for and against ","tagid":"456","tagName":"Clip closure of resection defect for risk of delayed bleeding"},{"id":"113","split":"1","chapterid":"216","timeFrom":"1060.64999","timeTo":"1265.984 ","number":"16","chaptername":"Technique for thermal ablation of the post EMR margin ","description":"The technique for margin ablation involves\n- keeping the catheter still\n- perfecting your tip control\n- creating a 1mm rim of ablated tissue around the full circumference of the lesion\n\n- recent data suggests that incomplete margin ablation removes the protective effect of the technique at surveillance endoscopy ","tagid":"273","tagName":"Thermal ablation of the post-polypectomy margin"},{"id":"113","split":"1","chapterid":"217","timeFrom":"1265.985 ","timeTo":"1389.592 ","number":"17","chaptername":"Technique for clip closure of the post-EMR defect ","description":"No deep injury is demonstrated within this defect (DMI type 0). The clip closure is for risk of bleeding (proximal colonic lesion).\n\nThe technique for clip closure is discussed\n- planning, (difficult to easy, left to right)\n- placement\n- rotation\n- suction and closure ","tagid":"456","tagName":"Clip closure of resection defect for risk of delayed bleeding"},{"id":"113","split":"1","chapterid":"218","timeFrom":"1389.593 ","timeTo":"1500.373 ","number":"18","chaptername":"Feedback on performance ","description":"Done well\n- tip control, margin ablation\n\n\nCould improve\n- lesion assessment\n- lifting, stab and pull back\n- avoid capture of tissue over folds\n- placement of clips ","tagid":"456","tagName":"Clip closure of resection defect for risk of delayed bleeding"}]
[{"name":"Polypectomy training, 20mm proximal transverse LSL","description":"Training of a colleague with some experience taking his next steps in polypectomy of an advanced lesion in the proximal transverse","summary":"","detailedSummary":"","author":"David Tate","tagger":"","editor":"","recorder":"","authorid":"1","centreName":"University Hospital of Ghent","centreCity":"Ghent","centreCountry":"Belgium"}]
[{"chapterTagid":"387","tagName":"Blunt injection","id":"452"},{"chapterTagid":"375","tagName":"Choice of snare type","id":"444"},{"chapterTagid":"399","tagName":"Clip closure of resection defect for risk of delayed bleeding","id":"456"},{"chapterTagid":"369","tagName":"Colon","id":"264"},{"chapterTagid":"389","tagName":"Dynamic injection","id":"453"},{"chapterTagid":"374","tagName":"En bloc versus piecemeal resection","id":"445"},{"chapterTagid":"371","tagName":"Endoscopic Mucosal Resection (piecemeal)","id":"294"},{"chapterTagid":"395","tagName":"Endoscopic Video and Room Video with Audio Plus Trainee","id":"462"},{"chapterTagid":"376","tagName":"Hot versus cold snare polypectomy","id":"446"},{"chapterTagid":"373","tagName":"Injection technique","id":"269"},{"chapterTagid":"366","tagName":"Kudo Classification","id":"302"},{"chapterTagid":"372","tagName":"Large (20mm or larger)","id":"289"},{"chapterTagid":"367","tagName":"NICE classification","id":"301"},{"chapterTagid":"370","tagName":"Non-granular","id":"309"},{"chapterTagid":"368","tagName":"Paris 0-IIa","id":"323"},{"chapterTagid":"382","tagName":"Post polypectomy defect assessment","id":"272"},{"chapterTagid":"380","tagName":"Safety checks prior to application of diathermy","id":"271"},{"chapterTagid":"381","tagName":"Snare placement","id":"270"},{"chapterTagid":"388","tagName":"Stab and pull back to find submucosal plane","id":"454"},{"chapterTagid":"397","tagName":"Submucosal adipose tissue","id":"461"},{"chapterTagid":"398","tagName":"Submucosal blood vessels","id":"458"},{"chapterTagid":"400","tagName":"Thermal ablation of the post-polypectomy margin","id":"273"},{"chapterTagid":"365","tagName":"Virtual chromoendoscopy","id":"306"},{"chapterTagid":"379","tagName":"[low risk] Right colon, flat, no nodules","id":"447"}]
Choice of snare typeEn bloc versus piecemeal resectionHot versus cold snare polypectomy
Deconstructed Polypectomy Technique
Injection techniquePost polypectomy defect assessmentSafety checks prior to application of diathermySnare placementThermal ablation of the post-polypectomy margin
Defect inspection deconstructed
Submucosal adipose tissueSubmucosal blood vessels
Endoscopic Markers of Submucosal Invasion [colon]
[low risk] Right colon, flat, no nodules
Gastrointestinal Location
Colon
Granularity
Non-granular
Imaging Classifications for Colorectal Polyps
Kudo ClassificationNICE classification
Imaging modalities
Virtual chromoendoscopy
Paris Classification
Paris 0-IIa
Polyp Size
Large (20mm or larger)
Polypectomy technique
Endoscopic Mucosal Resection (piecemeal)
Prevention of adverse events at polypectomy
Clip closure of resection defect for risk of delayed bleeding
Submucosal Injection Technique
Blunt injectionDynamic injectionStab and pull back to find submucosal plane
Video Type
Endoscopic Video and Room Video with Audio Plus Trainee
Registration will open in late January 2020. Prior to this you
can register your interest below and we will keep you updated on everything GIEQs.Your email address will only be used to update you on GIEQs
Join us for GIEQs II
Released prior to the early bird deadline these 6, 1-2 minute video
snippets
demonstrate the attention to detail, deconstructed approach and rock solid evidence
base of the GIEQs Approach.
1 - Over the Scope Clip for Upper
Gastrointestinal Bleeding Use of
OTSC as first-line for life
threatening upper gastrointestinal haemorrhage.
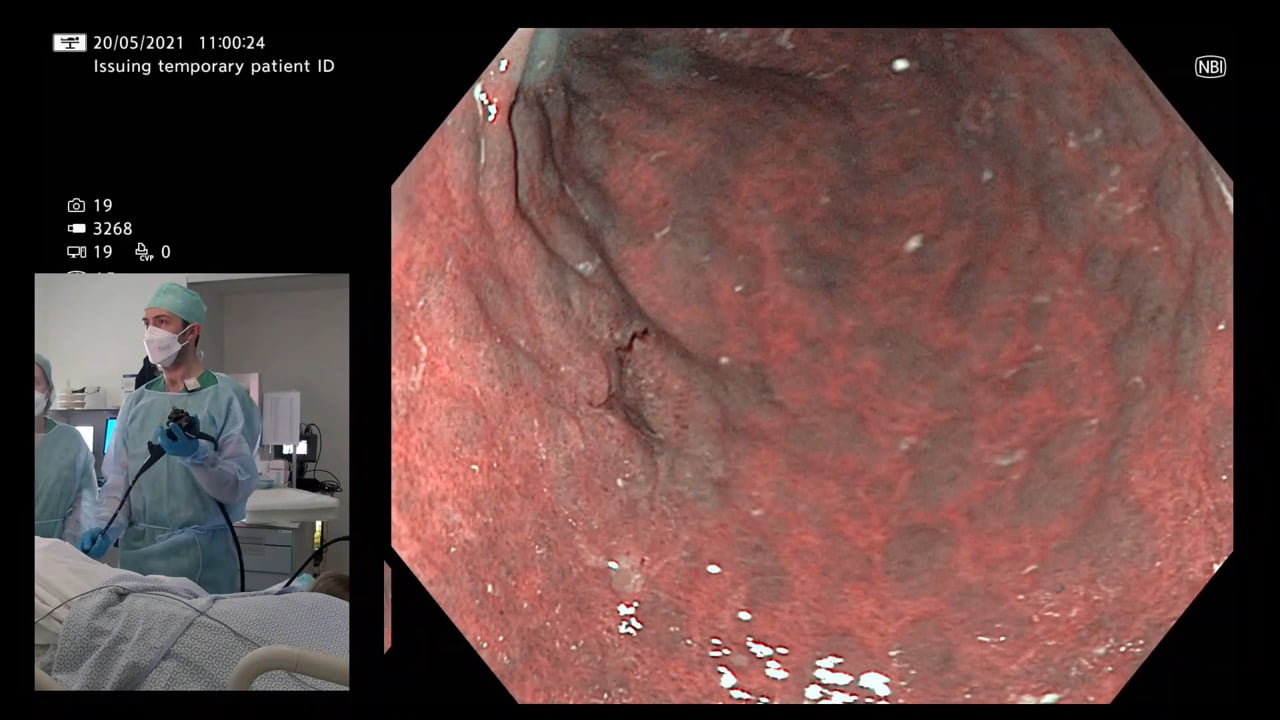
2 - Early Gastric Cancer Can you
identify and characterise
this early gastric cancer? Watch the video for more information
including endoscopic resectability
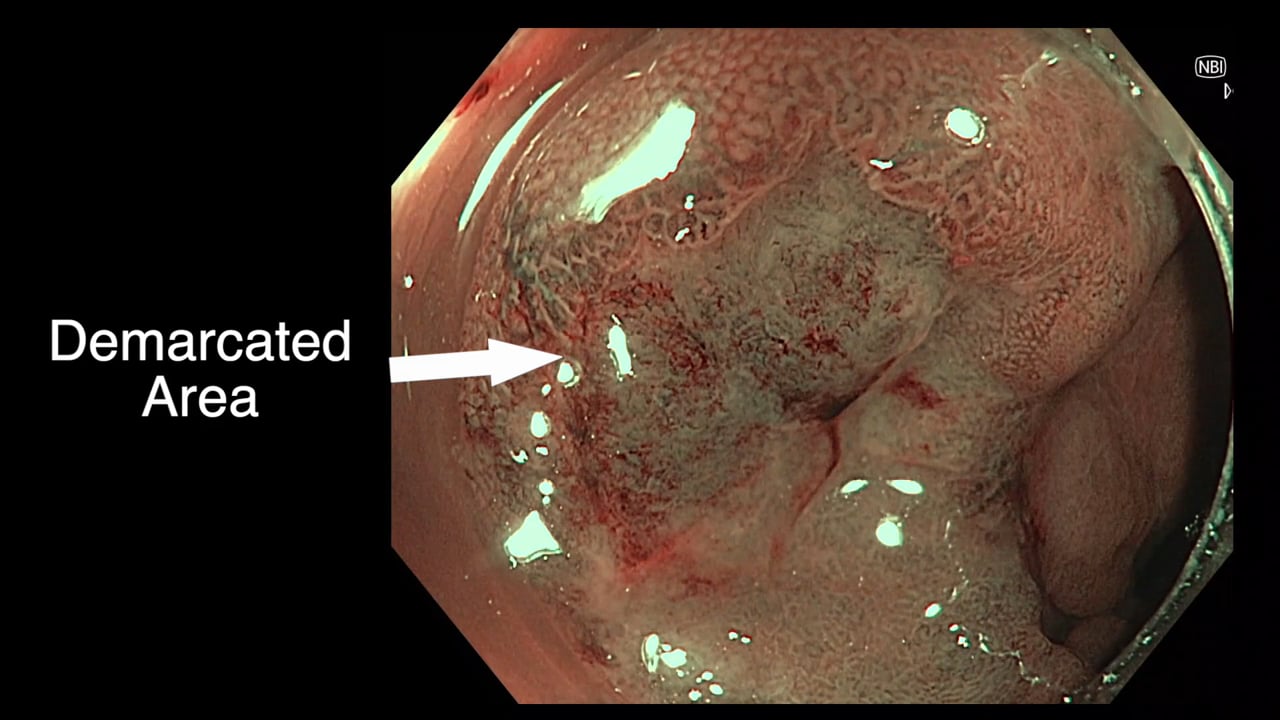
3 - The Demarcated Area as a Predictor of
Submucosal Invasion in Colon Polyps the Demarcated Area has emerged as a stable predictor
of submucosal invasive cancer. Find out more here.
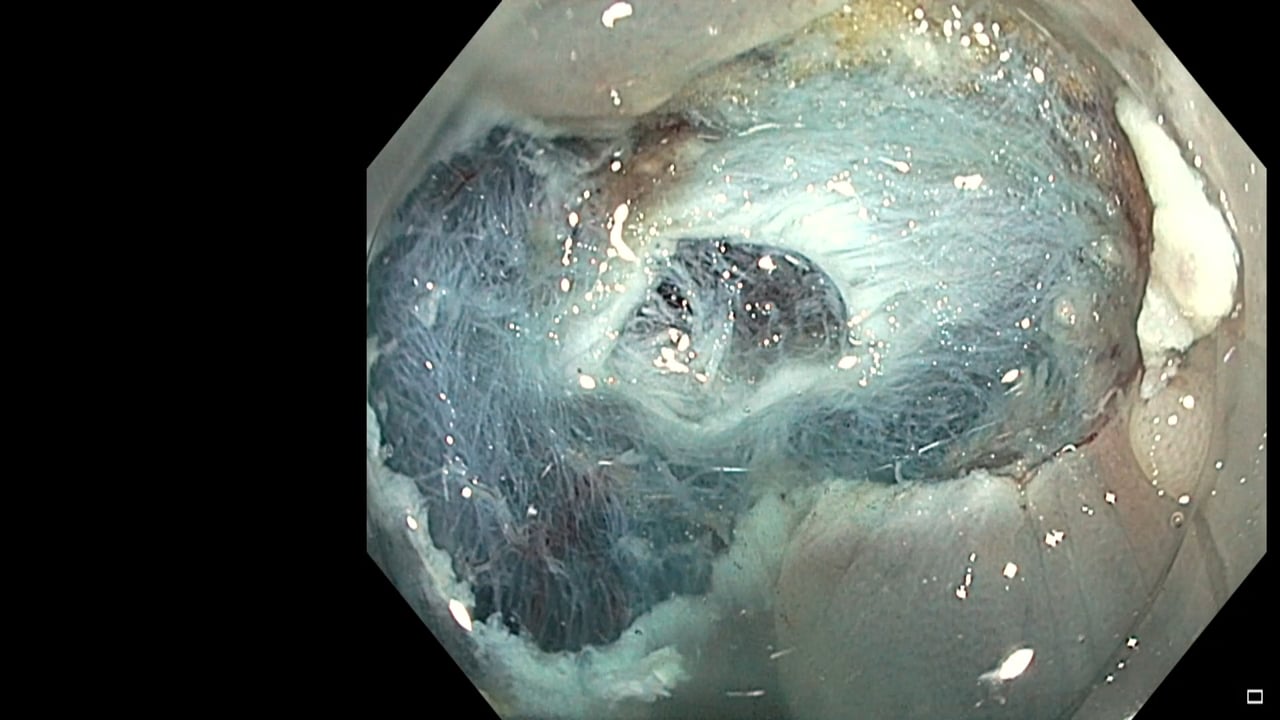
4 - Dealing with Adverse Events at Colonic
Polypectomy
To be able to competently perform colonic polypectomy you must be able
to deal with adverse events. A deconstructed example is shown
here.
5 - Complex EUS applications to make Everyday
ERCP easier Endoscopic Ultrasound
is radically changing the way we approach biliary intervention and can
make a difference to everyday endoscopic problems.
6 - Decision Making after Large perforation and
life threatening Bleeding during Polypectomy Many of the GIEQs faculty spend their normal working
lives on complex endoscopy. Learning the lessons and approach from these
procedures, deconstructing them and bringing them to the everyday is a
crucial part of the GIEQs approach.